Differential pressure gauges used in facilities complying with FDA CGMP should be suitable for their intended use, range and accuracy. They must be correctly installed, calibrated, alarmed and documented, while critical aseptic pressure points may require continuous electronic monitoring.
- Is there such a thing as an “FDA-approved factory”?
- FDA requirements for air-pressure control
- Does FDA specify a required pressure difference?
- Suitability for intended use
- Measuring-range selection
- Accuracy and resolution
- Mechanical or electronic instrumentation
- Continuous monitoring
- Alarm configuration
- Calibration requirements
- Calibration frequency
- Failed calibration
- BMS and EMS integration
- When does 21 CFR Part 11 apply?
- Installation considerations
- FAT, IQ and OQ
- HEPA filter pressure monitoring
- Inspection documentation
- Frequently asked questions
- Conclusion
Is there such a thing as an “FDA-approved factory”?
The phrase “FDA-approved factory” is widely used commercially but does not accurately describe the way FDA regulates manufacturing establishments.
FDA does not independently approve manufacturing facilities as a general certification. Facilities may be registered, inspected or evaluated in connection with a product application, but registration does not indicate FDA approval of the establishment or its products. More accurate descriptions include an FDA-registered facility, an FDA-inspected facility or a facility operating in compliance with applicable FDA CGMP requirements.
This article focuses on differential pressure gauges used in pharmaceutical facilities subject to 21 CFR Parts 210 and 211. Food, dietary supplement, cosmetic and medical-device facilities may be subject to different regulatory frameworks.

FDA requirements for air-pressure control
21 CFR 211.46 requires appropriate equipment for controlling air pressure, microorganisms, dust, humidity and temperature where these parameters are relevant to drug manufacturing, processing, packing or holding.
For aseptic processing, 21 CFR 211.42 requires HEPA-filtered air supplied under positive pressure, a system for monitoring environmental conditions and a system for maintaining equipment used to control aseptic conditions.
A differential pressure gauge is one part of this control system. It does not create FDA compliance by itself, but it provides evidence that the HVAC system is maintaining the approved pressure relationship and airflow direction.
Does FDA specify a required pressure difference?
FDA CGMP does not establish one pressure value for every cleanroom.
FDA’s aseptic-processing guidance recommends a positive differential of at least approximately 10–15 Pa between adjacent rooms of different classifications with the doors closed. It also gives an example of a substantial overpressure of at least approximately 12.5 Pa between an aseptic-processing room and an adjacent unclassified room. These are guidance recommendations rather than universal mandatory values for all facilities.
The final setpoint should reflect cleanroom classification, product risk, contamination-control objectives, containment requirements, door operation and qualification results.
Negative pressure may be appropriate for potent, toxic or dust-generating materials where containment and operator protection are required.
Suitability for intended use
The first step is to define whether the instrument will monitor room pressure, filter loading or duct pressure.
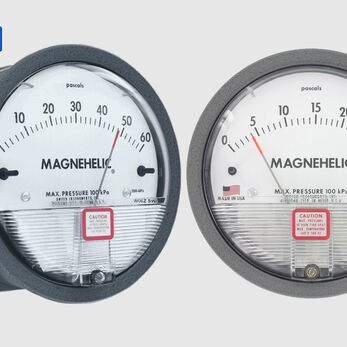
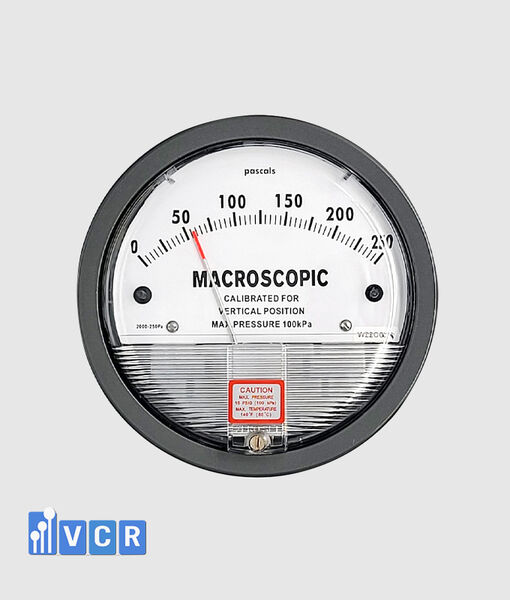
Room-pressure gauges normally operate at low values and require sufficient resolution to show small changes. HEPA, bag-filter and AHU-filter measurements usually require wider ranges.
A 0–1,000 Pa gauge may be suitable for filters but may provide poor readability for a room operating at only a few tens of pascals. A 0–60 Pa gauge may suit room pressure but can be exceeded in a filter application.
Under 21 CFR 211.68, automatic, mechanical and electronic equipment used in drug manufacturing must perform its intended function satisfactorily and be routinely calibrated, inspected or checked under a written programme.
Measuring-range selection
FDA does not prescribe a specific range such as 0–60 Pa, 0–125 Pa or 0–500 Pa.
Low ranges may be considered for room pressure. Filter applications may require ranges such as 0–250 Pa, 0–500 Pa, 0–750 Pa or 0–1,000 Pa, depending on initial resistance, final resistance and design airflow.
The selected range should exceed the maximum expected value but should not be unnecessarily wide.
The normal operating zone should be clearly readable rather than being located very close to zero or the full-scale limit.
Accuracy and resolution
FDA does not assign one accuracy class to all differential pressure gauges.
The instrument should be accurate enough to distinguish normal conditions from alert and action conditions.
Where the operating window is narrow, a gauge whose uncertainty is large compared with the control limits is not technically suitable, even when it is supplied with certificates of origin and quality.
Specifications should consider whether accuracy is expressed as a percentage of full scale or of reading. Resolution, repeatability, hysteresis, zero drift, temperature effect, mounting orientation and overpressure capability should also be evaluated.
Mechanical or electronic instrumentation
A mechanical pointer gauge is suitable for local indication. It normally requires no external power and can remain visible during a control-system power interruption.
A basic mechanical gauge cannot automatically log data or generate a remote alarm. It also provides no evidence of pressure behaviour between manual observations.
Electronic transmitters are more appropriate when alarms, trend records, HMI display or BMS/EMS integration are required. Common outputs include 4–20 mA, 0–10 V, RS485 and Modbus.
Critical points may use both a local mechanical gauge and an electronic transmitter. Each measurement path still requires appropriate calibration and verification.
Continuous monitoring
FDA’s aseptic-processing guidance recommends that pressure differences between cleanrooms be monitored continuously throughout each production shift and frequently recorded. Alarms should be documented, and departures from established limits should be investigated.
Monitoring criticality should be risk-based. Higher-priority points commonly include pressure relationships between aseptic rooms and backgrounds, between different cleanroom classifications, and between isolators and surrounding environments.
A lower-risk maintenance point, such as a pre-filter, may remain locally indicated when the approved inspection frequency provides adequate control.
Alarm configuration
The monitoring system should detect a developing low-pressure condition before lower-quality air enters the classified room. FDA recommends pressure specifications and alarms capable of rapidly detecting atypical environmental changes.
Alarm configuration should define low and, where relevant, high limits, delay time, hysteresis and the required operator response.
A delay can prevent nuisance alarms during short door openings, but an excessive delay may conceal a genuine deviation.
The system should distinguish a valid low-pressure condition from sensor power loss, broken wiring, communication failure or an out-of-range signal.
Calibration requirements
21 CFR 211.160 requires instruments, apparatus, gauges and recording devices to be calibrated at suitable intervals under an established written programme.
The programme must contain specific instructions, schedules, accuracy and precision limits and provisions for remedial action when limits are not met. Instruments that fail established specifications must not be used.
Calibration is more than adjusting the pointer to zero. The device should be compared with a suitable reference source at several points across its measuring range.
Mechanical gauges should be evaluated for increasing and decreasing pressure, repeatability, hysteresis and return to zero.
Electronic transmitters should be checked for applied pressure, local display, 4–20 mA or 0–10 V output and the value received by the PLC, BMS or EMS.
21 CFR 211.194 requires complete records of periodic calibration for applicable instruments, gauges and recording devices.
Calibration frequency
FDA does not require every differential pressure gauge to be calibrated at a fixed six-month or twelve-month interval.
The interval should be defined and justified using measurement criticality, manufacturer recommendations, operating conditions and historical calibration performance.
A device showing recurring drift may require a shorter interval. A stable history may support a risk-based interval review through change control.
FDA’s process-validation guidance also recommends maintaining qualified status through ongoing monitoring, maintenance and calibration and adjusting maintenance and calibration frequencies using feedback from those activities.
Failed calibration
An out-of-tolerance calibration result should not be addressed only by adjustment and return to service.
The facility should assess when the device may have become inaccurate, which records or batches may have been affected and whether pressure-control alarms remained reliable.
The assessment period commonly extends back to the most recent acceptable calibration unless other evidence supports a shorter period.
Actions may include repair, replacement, recalibration, interval reduction, product-impact assessment and CAPA.
BMS and EMS integration
Not every pressure gauge must be connected to a BMS or EMS. Critical points, however, should have an appropriate electronic method for alarms and records.
A BMS is commonly used for HVAC operation and fan or damper control. An EMS normally focuses on environmental records, alarm management and quality investigations.
Where BMS or EMS information is relied upon as a CGMP record, the system must control access, data accuracy, backup, retention and protection.
21 CFR 211.68 requires controls over computer systems, accuracy checks of input and output data, and backup data protected from alteration, inadvertent erasure or loss.
When does 21 CFR Part 11 apply?
21 CFR Part 11 should be considered when electronic records and electronic signatures are used to meet FDA record requirements.
For closed systems, 21 CFR 11.10 requires system validation, accurate and complete record copies, record protection, restricted access and secure time-stamped audit trails that capture the creation, modification and deletion of electronic records.
FDA’s data-integrity guidance states that CGMP data should be reliable and accurate and that firms should implement risk-based controls suited to their processes and technology.
A sensor with 4–20 mA output is not, by itself, “Part 11 compliant.” Compliance depends on the complete electronic record system, including software validation, user access, audit trails, backup, time synchronisation and change control.
Installation considerations
The High port should connect to the higher-pressure location and the Low port to the lower-pressure location.
Across a filter, High is upstream and Low is downstream. Between rooms, the connections depend on the intended pressure cascade and display convention.
Pressure taps should represent static pressure and should be positioned away from supply diffusers, return grilles, fans and dampers where dynamic pressure and turbulence may distort the measurement.
Tubing must be airtight, free from kinks and protected from condensation. High and Low lines should be clearly identified.
Mechanical gauges should be installed in the manufacturer’s specified orientation because mounting position can affect zero on some instruments.
FAT, IQ and OQ
FAT should verify the approved model, range, unit, accuracy, power supply, output and alarm functions.
For a 4–20 mA transmitter, several pressure points should be simulated to verify the relationship between applied pressure, current output and PLC or HMI indication.
IQ confirms that the correct device has been installed in the approved location with correct High–Low tubing, wiring, identification and calibration documentation.
OQ should challenge zero, multiple points, low and high alarms, delay, hysteresis, power loss, broken wiring and communication failure.
Where pressure feedback controls a fan or damper, the complete control loop should be challenged rather than only the sensor.
FDA’s process-validation guidance states that qualified status should be maintained through routine monitoring, maintenance and calibration, with periodic review to determine whether requalification is necessary.
HEPA filter pressure monitoring
A HEPA differential pressure gauge should cover the range from clean-filter resistance to the approved final operating limit.
Readings should be compared at similar airflow conditions. Lower fan speed may reduce pressure drop even when the filter is loaded, while increasing fan speed may raise pressure drop.
Differential pressure does not demonstrate HEPA integrity. Torn media, seal leakage or bypass may still produce a pressure reading. Filter integrity requires an appropriate HEPA leak test.
Replacement limits should be based on the filter datasheet, qualified airflow, fan capability and approved system limits rather than one universal value.
Inspection documentation
Documentation should demonstrate the complete lifecycle of each important differential pressure point.
Typical documents include the URS, risk assessment, datasheet, pressure-tapping drawings, instrument list, FAT, IQ, OQ, calibration certificates, operating procedures, alarm-response procedures, maintenance records and deviation history.
Electronic systems should also include scaling configuration, alarm lists, user access, audit trails, backup and recovery, change control and periodic review.
FDA inspection readiness requires more than a reasonable value appearing on the gauge during the inspection. The facility should demonstrate that the instrument was properly specified, qualified, calibrated and maintained in a state of control.
Frequently asked questions
Does FDA specify an approved gauge brand?
No. FDA focuses on suitability for intended use, performance, calibration, inspection and supporting records.
Can a mechanical gauge be used?
Yes. A mechanical gauge can be suitable for local indication when its range, accuracy, calibration and record procedure are appropriate. Critical continuously monitored points normally require an electronic transmitter.
Is 10–15 Pa mandatory for every cleanroom?
No. FDA presents 10–15 Pa as a recommendation for adjacent rooms of different classifications in aseptic processing. The actual value should be established and qualified for the facility.
Is EMS integration mandatory?
Not for every point. Critical measurements requiring continuous alarms and records need an appropriate electronic solution.
Is annual calibration mandatory?
No. FDA requires a defined and suitable interval under a written programme. The interval should be justified through risk and historical performance.
Is a 4–20 mA device automatically compliant with Part 11?
No. Part 11 relates to the complete electronic-record system, including validation, access control, audit trails, record protection and retrieval.
Conclusion
A differential pressure gauge in an FDA CGMP facility should be managed as part of the environmental and HVAC control system, not merely as a wall-mounted indicator.
The device should have a defined intended use, appropriate range, resolution and accuracy. Pressure taps, High–Low connections and tubing should be correctly installed. Operating limits, alarms and responses should be established and qualified.
Gauges and transmitters require calibration under a written programme with acceptance limits and remedial actions. Critical measurements should be continuously monitored, recorded and alarmed where necessary.
When data are stored in a BMS or EMS, the facility should address 21 CFR 211.68, 21 CFR Part 11 and FDA data-integrity expectations. A digital display or 4–20 mA output alone does not establish compliance.
VCR Cleanroom Equipment supplies mechanical differential pressure gauges, electronic indicators and transmitters with 4–20 mA, 0–10 V and Modbus outputs for cleanrooms, AHUs, HEPA boxes, pass boxes, air showers, FFUs, laminar airflow units and dispensing booths. VCR also supports range selection, alarm configuration, calibration, loop checks and FAT, IQ and OQ documentation.